


Medical Home Overall Goal
By September 30, 2020, increase the number of children and youth with special health care needs (CYSHCN) who receive family-centered, coordinated, comprehensive, culturally appropriate and continuous care within a medical home.
Medical Home Overall Strategy
Enhance capacity (infrastructure) and support community-based organizations that promote medical homes for CYSHCN and their families, which blend systems principles, standards and measures with National Standards for Systems of Care for CYSHCN around CYSHCN domains that include Medical Home, Care Coordination, Community-Based Services and Supports, Family-Professional Partnerships and Transition to Adulthood.
Objective CS-1: Care Coordination
By September 30, 2020, increase the number of CYSHCN who have access to care coordination within a medical home.
Strategy CS-1.1: Improve identification of CYSHCN in Medicaid Managed Care Plans
Increase the percent of Medicaid-enrolled children and youth with special health care needs receiving services funded by the state Title V CYSHCN program whose records are matched with the state Medicaid (Health Care Authority [HCA]) database and flagged to activate comprehensive services with care coordination within their health plan.
- Update the Child Health Intake Form (CHIF) process, shown below, to include collection of ProviderOne numbers for those children and youth with special health care needs enrolled in Medicaid. COMPLETED
- Complete redesign of the CHIF system to improve the transfer of CHIF data to HCA.
- Update interagency data sharing agreement and continue quarterly data sharing with HCA to assist in identification of CYSHCN for health plan-level care coordination. COMPLETED
- Monitor data to determine if the number of children flagged in ProviderOne has increased over baseline (quality improvement/quality assurance).
- Work strategically on educating the managed care organizations (MCOs) on the importance of this new flag in Medicaid’s Predictive Risk Intelligence SysteM (PRISM).

- Continue to work with neurodevelopmental centers (NDCs) to increase the number of CYSHCN they serve whose records they send to local health jurisdictions (LHJs) to be CHIF’d. Once the CHIF redesign is complete (during federal fiscal year [FFY] 2019 or 2020), NDCs will have access to enter records for the children they serve directly into the CHIF database instead of sending the information to LHJs for them to enter. We anticipate this will increase the number of CYSHCN NDCs serve that end up in the CHIF database. In addition, we will shift the NDC state match funds from supporting transition into managed care (completed) to increase organizational capacity and workforce development activities in FFY 2020.
- Our evidence-based strategy measure (ESM) for medical home is the percentage of Medicaid-enrolled CYSHCN receiving services whose records are matched with the HCA database. Proper matching will help facilitate the appropriate care for these individuals within a medical home model. At baseline in 2016, an estimated 50 percent of records were matched. Our goal was to increase this percentage to 100 percent by the end of FFY 2020. For calendar year 2018, we found that 99.8 percent of children had their records matched.
With the CHIF redesign, we anticipate some new short-term challenges with data-matching. We expect to work through these as we test and use the new database.
Strategy CS-1.2: Promote integration of care through effective and timely information sharing
Identify state-specific activities to promote integration of care for CYSHCN for physical, oral and mental health with other primary and specialty providers and ensure that information is shared effectively with families and among and between providers, which includes shared management of CYSHCN between pediatric primary care and specialty providers and families’ access to care plans.
- Work with public and private health plans to implement policies and procedures. Our goal is to ensure that information is shared effectively with families, and among and between providers and programs serving CYSHCN and their families. In FFY 2020, we will initiate some connections to military systems and identify ways to influence better care coordination for families served in military-funded health systems and those families enrolled in the Exceptional Family Member Program.
- Continue to contract with partners who promote coordination between referral entities and improve evaluation of those activities. The University of Washington (UW) Medical Home Partnerships Project (MHPP) has a new website which serves as a resource to educate providers, families, and community partners on medical home and care coordination resources. In FFY 2020 the CYSHCN program will streamline the work of the MHPP contract by leveraging their relationship to the UW Leadership Education in Neurodevelopmental and Related Disabilities (LEND) program. We expect to create a stronger focus of work that includes partnering with the Washington Chapter of the American Academy of Pediatrics (WCAAP) to identify workforce development and technical assistance strategies to support primary care providers that offer medical home and care coordination services.
- Collaborate with partners including WCAAP to educate and support clinicians on effective care integration and cross-provider communication through training and access to tools and materials. Promote and support the use of telehealth to increase access to underserved communities.
- Explore other populations for inclusion in the CHIF system. Pilot the CHIF database as a way to model evidence-based program planning and decision making, and workforce development planning.
Strategy CS-1.3: Promote multi-disciplinary care
Provide the supports necessary for training and development of multi-disciplinary care teams within the medical home model (including the use of family-centered, coordinated, ongoing comprehensive care) to ensure coordination across clinics, hospitals, schools, social services and community-based preventive resources to promote quality of life, healthy development and healthy behaviors across all life stages.
- Support or promote referrals and linkages to effective and evidence-based services through contracts with NDCs and maxillofacial review boards (contracts funded with state general funds, with contract management and staff support funded through MCHBG), and a contract with UW to train nutritionists, registered dietitian nutritionists (RDNs) and interdisciplinary community-based feeding teams.
- Explore ways, such as a self-assessment on use of shared plans of care, to support coordination with specialty pediatric centers of care (e.g., pulmonary, maxillofacial, newborn screening, newborn hearing screening, Autism Centers of Excellence, CYSHCN coordinators, UW LEND, and NDCs) for CYSHCN and their families.
- Explore opportunities to collaborate with partners, including other Department of Health (DOH) programs and other state agencies to support increased use of telemedicine, consultative models, and other electronic communications to enhance access to pediatric specialty care and ancillary services for CYSHCN, particularly those living in rural areas.
Strategy CS-1.4: Promote use of shared plans of care (SPOC)
Educate and support providers and care coordinators from across systems on best practices in providing care coordination for children through training and access to tools, including shared plans of care. Use a quality improvement approach to increase the percent of children in the maxillofacial program who have a documented SPOC that follows the Packard standards.
This strategy and all related activities were completed during FFY 2017 with funding and staff support from the Great LINCS (Links to Integrate and Coordinate Services) discretionary grant, and staff and contract funds from federal MCHBG and state funds.
Strategy CS-1.5: Increase provider capacity to provide culturally and linguistically appropriate care coordination
Promote and support culturally and linguistically appropriate care coordination within the medical home to connect children and families to comprehensive medical care and community resources.
We will continue to provide support for workforce development and training to ensure that providers are skilled in meeting the cultural, linguistic and disability-specific needs of CYSHCN and their families. In FFY 2020 we will use the CHIF demographic data to try to interpret the impact of targeted outreach by NDCs to provide materials in multiple languages to underserved communities. State match funds will be available to translate outreach materials to culturally and linguistically diverse audiences who need therapeutic services.
Status to Date and Upcoming Plans for Objective CS-1
The addition of the CYSHCN indicator to PRISM allows MCOs to sort client data specifically to identify CYSHCN; MCOs can then offer the family enhanced care coordination through their health plan. Prior to this enhancement, MCOs had no way to reliably identify CYSHCN in their data system. We worked with the Department of Social and Health Services (DSHS) to add the CYSHCN indicator to each client’s file to enable all MCO case managers access to this information. Trainings were conducted in FFY 2016 with occasional technical assistance provided in FFY 2018. Following the deployment of the new CHIF database, the CYSHCN program will assess the effectiveness of the PRISM flag to effectively trigger enhanced care coordination services from MCO coordinators.
Through the UW MHPP contract, MCHBG funding is used to share information related to medical homes with a wide network of primary care providers (PCPs) and other members of medical home teams through the Medical Home Leadership Network via newsletters and Child Health Notes. During FFY 2019, MCHBG-funded staff from several programs at DOH are providing support to this.
Pediatric – Transforming Clinical Practice Initiative (P-TCPi) funding was braided into the UW MHPP contract to partner on two projects: Medical Home Neighborhood Team (MHNT) and Regional Care Coordination (RCC). The MHNT provides leadership, guidance, tools, and resources to clinicians and their practices working through practice transformation, to position those practices as sustainable components within the changing care delivery system.
The RCC project created a one-year statewide network of Regional Care Facilitators (RCFs), one in each of the state’s nine Accountable Communities of Health (ACHs), to support a system of care coordination that strengthens linkages between pediatric providers and improves health outcomes for children on Medicaid. These RCFs participated in broader P-TCPi initiative activities, including promotion of systems integration between primary and behavioral health, collaborating with MCOs to support care coordination, and partnering with P-TCPi practice facilitators and practices to build the Medical Home Neighborhood model.
Although P-TCPi funding for the RCC project was only available during FFY 2018, the CYSHCN program is partnering with UW MHPP to identify other means to sustain the RCF model. Some FFY 2019 Maternal and Child Health Block Grant (MCHBG) dollars were allocated to this work. The CYSHCN program will hold contract planning discussions with partners in summer 2019 to identify ways in which the MHPP contractor can continue to support WCAAP efforts to prepare the pediatric provider workforce for healthcare transformation. In 2019, the CYSHCN program also provided technical assistance to UW MHPP about framing their contracted work as a statewide technical assistance center for medical home and developmental screening, especially autism screening.
Community Asset Mapping (CAM) activities, part of the UW MHPP contract, promote and facilitate coordination between referral entities. CAM activities are funded through MCHBG funds as well as through the state’s Autism Spectrum Disorders and Other Developmental Disabilities (AS3D) grant, and will continue throughout FFY 2019. While the current autism grant will be completed in August 2019, many of the CAM communities have gained enough momentum to continue, and infrastructure is in place to support CAM communities. Additional details about CAM are provided in the CYSHCN Annual Report in the NPM 11 section on System Coordination and Collaboration.
Contract work with maxillofacial review boards (MFRBs) continues during FFY 2019 and FFY 2020 through contracts that include quality improvement activities for exploring sustainable funding sources for the care coordination provided by MFRBs. Although the MFRB contracts are funded with state general funds (match), these contracts are managed and supported by MCHBG-funded team members at DOH.
We are also continuing the UW statewide nutrition contract during FFY 2019 and FFY 2020, which focuses on workforce expansion and dissemination of available nutrition resources to many providers, including PCPs. Through this contract, as well as ongoing partnership with the Department of Children, Youth, and Families (DCYF), Smooth Way Home, the Washington Association for Infant Mental Health (WA-AIMH), families, and providers, regular meetings are convened to explore, refine and promote transition supports for fragile infants transitioning from hospital to home. The nutrition needs assessment completed in FFY 2018 and being finalized in 2019 indicated that a primary barrier to adequate nutrition services for CYSHCN was lack of referrals from primary care providers. For FFY 2020, the nutrition contract, the MHPP contract, and the LEND program, all located at UW, will collaborate to streamline their foci of work for their MCHGB contracts. They will include increasing needed referrals to registered dieticians who have the clinical expertise to address the often complex nutritional needs of CYSHCN, especially those with medical and behavioral complexity.
Through state general funds (match) and MCHBG-funded CYSHCN program staff, we continue to support interdisciplinary care at 19 NDCs across the state, where CYSHCN have access to multiple specialty services. The CYSHCN program is leveraging this investment to support expansion of available services for children with Medicaid at NDCs. The state fiscal year 2020 contract with the NDCs will include development of a work plan and implementation plan to increase capacity to serve rural and underserved CYSHCN through a variety of workforce development and infrastructure building activities. Examples include increasing outreach to culturally diverse communities, enhancing access through telehealth infrastructure building, offering preceptor and externships to increase provider base, and other projects as identified.
The NDCs will also use CHIF data to conduct continuous quality improvement around their targeted populations served. This type of systems-building work and leveraging of multiple funding streams is facilitated through the leadership, technical assistance and coordination provided by MCHBG-funded CYSHCN program staff.
Additional current and upcoming work regarding multi- and inter-disciplinary care for CYSHCN includes participation in the national Collaborative for Improvement and Innovation Network (CoIIN) to Advance Care for Children with Medical Complexity (CMC). The CMC CoIIN is a four-year project funded by the Health Resources and Services Administration (HRSA) Maternal and Child Health Bureau, and Washington State has been chosen by the Center for Advancing Health Policy and Practice, Boston University School of Public Health, who leads the CoIIN, as one of 10 state teams partnering in this effort.
The CMC CoIIN seeks to improve the quality of life for CMC, the wellbeing of their families, and the cost-effectiveness of their care through development and implementation of innovative care and payment models. As part of Washington’s project team, the CYSHCN program provides support from staff funded by both federal MCHBG funds and state funds. The team is currently led by Seattle Children’s Hospital, who is the principal investigator (PI) and recipient of a subcontract from the Center for Advancing Health Policy and Practice. Through the subcontract, support will also be provided to PAVE (Partnerships for Action, Voices for Empowerment), which is Washington’s Title V designated Family to Family Health Information Center. The CYSHCN program has already played a critical role in this project – we successfully applied for participation, organized and led the state’s team early in the project, selected the PI, and provided technical assistance to the PI in negotiating the subcontract with the Center for Advancing Health Policy and Practice.
The state’s team plans to concentrate on babies discharging from the neonatal intensive-care unit (NICU), with special focus on clinically complex infants with feeding tubes, to ensure they receive adequate support as they transition to home from the NICU. The project funds a family navigator to follow up with families at three months, six months, nine months, and one year of age to ensure the families are connected to needed resources, that they are enrolled in a medical home, and to collect data about their experiences with family-centered care and integration of services. We plan to leverage long-term Title V CYSHCN investments in the statewide nutrition network and feeding teams in this work, and our nutrition contractor participates in the state team to maximize referral needs to appropriate community-based nutrition services.
During FFY 2018, CYSHCN program staff participated in training on Cultural Humility, provided through Maternal and Child Health Bureau technical assistance. Also during FFY 2018 and FFY 2019, through the AS3D grant, staff are working with HCA’s interpreter services program, the Northwest Autism Center (service provider in Spokane), and Open Doors for Multicultural Families, to address technical assistance and educational needs. Expected activities include a family-centered infographic that explains telehealth, provider training and educating the Medicaid-contracted interpreter brokers on telehealth. For FFY 2020, the CYSHCN program will engage in additional strategic planning around how the use of telehealth and an increased focus on workforce development activities can be incorporated into the priority setting of the MCHBG needs assessment to use innovative strategies and improve equity for the next five-year cycle.
Objective CS-2: Family Professional Partnerships and Family Engagement
By September 30, 2020, increase the number of family members of CYSHCN (including children with hearing loss) who are trained, engaged, supported and involved at all levels of program planning and implementation and who are satisfied with the health care and related services that their children are receiving. Create and maintain an effective statewide, cross-partner system to: (1) engage and train families of children and youth with special health care needs, and (2) connect trained family leaders to opportunities to advise, advocate and lead efforts to improve health and related systems of care at the individual, community, state and federal levels of systems development and improvement.
Strategy CS-2.1
Strengthen statewide capacity for parent/family training and support. Prepare families and youth to be active participants in improving systems of care by supporting the infrastructure for and providing technical assistance to programs and/or organizations that provide culturally appropriate family and youth leadership training in advisory and advocacy skills and peer support.
- Evaluate contracted partners’ existing family/parent training programs and curricula for effectiveness and relevance. Both the Washington State Fathers Network (WSFN) and all of the local Parent to Parent coordinators have taken the “Train the Trainer” version of Telling Your Story with a Purpose, and have been conducting the training around the state. Parents are offered a Washington State Leadership Initiative (WSLI) coalition “consent form” to be added to the communications list and receive the weekly newsletter to identify trainings and leadership opportunities. In FFY 2020 we will work with these contractors to try and determine the reach of these trainings. We would like to know how many of them have taken the training and then gone on to find additional leadership opportunities offered through the WSLI coalition.
- Continue to support existing parent support organizations such as Parent to Parent, Family to Family Health Information Center (F2FHIC), WSFN, and new partners to provide effective family and youth training in advisory, advocacy and peer support skills.
- Explore opportunities to create and promote parent leadership trainings across the state with state partners; explore possible unidentified parent support organizations that may benefit from partnership or technical assistance with DOH.
- Continue to actively recruit new parents for family leadership training.
- Explore options for increasing family input in small and rural counties.
Strategy CS-2.2
Strengthen statewide capacity to connect trained family leaders to advisory and advocacy opportunities.
- Create and maintain a cross-system, cross-partner mechanism to track up-to-date opportunities for family leaders to advise, advocate and lead efforts to improve health and related systems of care at the individual, community and state levels of systems development. In FFY 2020, will identify a strategy to use the analytics of the WSLI weekly newsletter to determine what types of training opportunities people are interested in, and use continuous quality improvement tools to inform content.
- Create and maintain a cross-system, cross-partner database of trained family leaders and their interest areas in order to recruit and connect them to relevant advisory, advocacy and peer support opportunities. At this time there are 952 individuals subscribed to the weekly newsletter, which can be sorted by county or topic of interest. There is not currently a mechanism to identify which trainings people have completed, however we can track interest levels through data analytics.
- Provide training for Title V staff on how to enhance family-professional partnerships within specific projects and activities. In FFY 2017, the Family Engagement Coordinator (FEC) led a Family and Consumer Partnership Business Analysis, utilizing the Association of Maternal and Child Health Programs (AMCHP) Levels of Family Engagement in Title V MCH and CYSHCN Programs as one of several resources. In FFY 2019 the FEC created a toolkit based on the business analysis. The toolkit will be promoted and used to promote implementation of family engagement and partnership strategies within Title V.
Strategy CS-2.3
Connect families of CYSHCN served across state agencies to family organizations, peer support and family support programs.
- Maintain strong relationships with Washington family organizations, peer support groups and family support programs.
- Include information about the availability of family organizations and peer and family support groups during parent trainings.
Strategy CS-2.4
Support and promote family professional partnerships and engagement through program planning and financial support in multiple programs and organizations.
- Partner with families/parents of CYSHCN from diverse backgrounds and experiences in designing and implementing DOH needs assessment activities for CYSHCN, and include findings from family surveys, focus groups and stories in strategic planning activities.
- Continue to provide reimbursement for parent involvement in DOH activities through the F2FHIC contract.
- Include the need for family participation in state contracts with our partners.
- Advocate and model for other state agencies the importance of reimbursement for family participation.
Status to Date and Upcoming Plans for Objective CS-2
Our Title V FEC will continue to lead the statewide family and consumer leadership network, the Washington Statewide Leadership Initiative coalition. Member organizations include community agencies that support families, and other state agencies that support family engagement. The goal is to increase opportunities for trained family leaders to participate and partner in strategic and program planning for systems improvement.
Federal MCHBG funds are used to support this effort, for staffing and contracted work. Additional funds from AS3D are used as well; family advisors and leaders from family-led organizations are a critical part of AS3D grant implementation. Family-led organizations who are also WSLI members include the Washington Autism Alliance and Advocacy, Open Doors for Multicultural Families, and the Northwest Autism Center. They are contracted partners in implementing the grant, are critical members of the grant’s project advisory committee, and they participate in WSLI activities on a regular basis.
During FFY 2019, the CYSHCN program made changes in our contracts with family-led organizations. Our contract with the state Parent to Parent (P2P) program consisted of funds allocated for state-level activities, as well as funds for the local P2P programs. The state legislature had voted to support P2P in all counties through their developmental disabilities system of care, increasing the number of local programs. The funds from MCHBG were increasingly spread more thinly to more organizations. This made program evaluation of the impacts of those investments difficult, as the burden of tracking and reporting outcomes became very high compared to the amount of funding each organization received.
Rather than continuing to contract with the state P2P program for pass-through to all the local programs, we made an amicable shift. We are providing the funds to increase the capacity of our F2FHIC, and included partnership funds in the form of grants to local P2P programs to allow the local communities to engage in collaborative projects with the support of the F2FHIC. It is our expectation this will strengthen the relationship between the two programs and provide mutual opportunities for each organization to leverage their expertise, networks and individual expertise.
The P2P program chose to use the MCHBG funds subcontracted from the F2FHIC to have all of the coordinators take a train-the-trainer course for Sibshops, a sibling support workshop program. This allows them to conduct Sibshops in their local communities, for siblings of CYSHCN to support and promote family resilience. In addition, as a result of the Sibshop training, many of the counties provided additional funding to the local programs to conduct some of their initial workshops.
MCHBG funds were also sub-contracted from PAVE to P2P programs for their annual statewide training conference. Both our F2FHIC and the P2P programs felt this strategy improved their ability to work with families and implement crucial community programs.
PAVE is a new contractor for DOH. Funds were allocated to increase the capacity of PAVE, which allowed them to hire additional staff to support the work of the WSLI coalition, manage the WSLI website and support the evaluation capacity of the statewide P2P program. As P2P is very connected to organizations serving people with developmental disabilities, it is our hope that by funding them through our partnership with PAVE, we can leverage PAVE’s Title V expertise as the F2FHIC to expand the P2P programs to better serve the broader CYSHCN population and to promote health equity and systems integration.
Washington State Fathers Network, supported through a Title V contract, currently has two formalized local chapters and a statewide steering committee comprised of six fathers. They also collaborate with other father-focused groups to conduct outreach to fathers across the state. During the FFY 2018 contract year, WSFN began to transition away from being a predominantly chapter-based organization to include increased social media support opportunities and regional dad volunteers who can take leadership roles in their communities to connect dads to opportunities identified by the WSFN and Father’s Alliance partners. They have increased their focus on the importance of fatherhood relationships for CYSHCN.
The WSFN contract deliverables included plan-do-study-act (PDSA) cycles around the program’s goals to increase online outreach to rural and underserved areas of the state through social media, utilizing online analytics to drive outreach. We also want to increase the number of fathers to join a “cadre” of men available to speak at conferences, panel discussions and events about the importance of father relationships for CYSHCN. Our contractor’s salary is 75 percent funded through MCHBG, so the majority of his program efforts are MCHBG work. Part of his time is spent serving on a steering committee for the Washington State Interagency Fatherhood Council, a program of Washington State Frontiers of Innovation. He provides training and orientation to fathers serving on the council to better equip them to “tell their story” and represent their lived experiences to improve social service systems. This Council aims to bring positive fatherhood perspective and relevance to services that can often be seen as “mom-centric,” such as child welfare, child support enforcement, and family economic support programs.
Many other groups conduct family outreach, including the Developmental Disabilities Council (DDC), many diagnosis-specific groups, Washington’s Parent Leadership Training Institute, Community Café Collaborative, and The Arc Parent Coalitions. We believe the creation of a statewide network infrastructure (WSLI) allows us to better track the work being done. In addition, the traditional model of peer-to-peer support does not always align with the needs of diverse families, and the WSLI partnerships allow us to exchange information and learn from each other. We also expand our family partnership goals beyond the CYSHCN priority area, as the different organizations involved serve all types of families, both with and without CYSHCN.
We have also increased collaboration with the DDC to use trained family advocates to model community inclusion and independence while simultaneously improving systems.
The FEC has been working with the MCH Workforce Development Center in 2018-19 on the implementation plan for the Family and Consumer Partnership Business Analysis. Together they co-presented the toolkit and implementation plan at the 2019 AMCHP conference to share it with others.
The CYSHCN program hired a new FEC in June 2019, and an important part of her work will be to become oriented to the toolkit and share it with partners. It is also our hope to adapt it so it can be used by different audiences. For example, rather than family engagement in Title V, we can adapt it to person and family engagement in primary practice using the same results based accountability and implementation science tools to adapt the toolkit content. More information on the work in Objective CS-2 can be found in the Family Partnership section.
Objective CS-3: System Coordination and Collaboration
By September 30, 2020, improve and promote systems of collaboration at the community level for effective service delivery across the health care system for CYSHCN (including Genetics and EHDDI [Early Hearing-loss Detection, Diagnosis and Intervention]) and their families between pediatric, family practice, and primary care medical homes, specialty care, hospitals, local health jurisdictions, community health centers and other children-serving entities to link families to community-based resources.
Strategy CS-3.1
(Using supplemental funding from a HRSA D70 Systems Integration Grant,) expand and support a centralized resource of information for families and providers of CYSHCN (including Genetics and EHDDI). By October 2017, 50 percent of families and medical home providers of CYSHCN contacting a shared resource for a needed specialist, support or service, will obtain a needed specialist, support, or service. COMPLETED
Strategy CS-3.2
(Using supplemental funding from a HRSA D70 Systems Integration Grant,) work with another state agency to improve the timely receipt of information following an initial referral of a CYSHCN by a medical home. Establish a written agreement and policy with the Department of Children, Youth and Families, Early Support for Infants and Toddlers (ESIT) program to improve the timely receipt of information following the initial referral of a CYSHCN by a medical home. COMPLETED in FFY 2016
Strategy CS-3.3
Continue to provide and participate in forums for infrastructure and systems development for CYSHCN (including Genetics and EHDDI).
- Continue to host the CYSHCN Communication Network meeting quarterly.
- Continue to promote networking among various and diverse entities by inviting a wide range of partners to the Communication Network, state and other planning meetings and workgroups; regularly explore new partners to include.
- Invite and include parents and families of CYSHCN to participate in state planning meetings and workgroups funded by MCHBG and supplemental grants funded by other sources.
- Support connections and networking between family organizations, care coordinators, providers and parent leaders.
- Use the aforementioned forums to work with community partners and stakeholders to identify gaps, prioritize needs and develop strategies for improvements.
Strategy CS-3.4
Provide technical assistance to support development of the medical home model.
- Maintain contracts and relationships with community partners, such as UW MHPP and WithinReach to support their efforts towards medical home promotion, including training to ensure better coordination for CYSHCN. In FFY 2020, as MHPP becomes more aligned with the UW LEND program, we will spend this last year of our current five-year plan identifying alignment and strategic planning to prepare for and move forward with the next five-year plan. UW MHPP has also expressed a desire to more strategically align their work with the higher-level goals of the CYSHCN program, the Office of Family and Community Health Improvement and DOH as a whole.
- Continue to support organizations participating in Community Asset Mapping. The SMART tool that several CAM communities are using has been very successful, and UW MHPP is partnering with Seattle Children’s Hospital to promote the SMART approach through their existing Project ECHO (Extension for Community Healthcare Outcomes) model. Seattle Children’s received a $150,000 grant to support SMART communities with ongoing training and support, and will identify a model to offer SMART teams virtually to support other rural communities in medically underserved areas.
- Increase access to care for CYSHCN in Washington by promoting use of telehealth. The general strategy of telehealth is being widely used by health centers to increase access to and improve quality of care. According to the Center for Connected Health Policy, telehealth encompasses a broad variety of technologies and tactics to deliver virtual medical, health and education services. Although increased use of telehealth is being seen primarily for adults with acute chronic conditions, this innovation can and should be used more widely in serving CYSHCN.
- Provide MCHBG-funded subject matter and program planning, implementation, and coordination expertise to Seattle Children’s Hospital, who leads Washington’s CMC CoIIN. This presents an unplanned yet fortuitous opportunity to coordinate and collaborate across systems (including Seattle Children’s health systems, managed care and Medicaid, the F2FHIC, the UW nutrition contract activities, and others) to increase access to medical homes and explore innovative coverage and payment models for CMC. This work also supports our adequate insurance priority area.
Strategy CS-3.5
Partner with local health jurisdictions’ (LHJ) CYSHCN and MCH programs to increase access to needed services for CYSHCN across the state.
- In partnership with LHJs, update the annual Focus of Work for CYSHCN contract document (which guides the MCHBG-funded contract work of LHJs on behalf of CYSHCN) to include additional information about the MCHBG and service levels (direct, enabling, public health/policy); organize the required strategies and activities by service level and include examples of the work LHJs are actually doing; and encourage exploration of regional coordination/collaboration.
- Provide additional ongoing opportunities for joint planning, brainstorming and problem solving, both between the state CYSHCN program and local CYSHCN programs, and between local CYSHCN programs.
Status to Date and Upcoming Plans for Objective CS-3
The CYSHCN Communication Network will include a new focus on engaging stakeholders in the CYSHCN portion of the MCHBG five-year needs assessment process. The intent is to identify gaps, prioritize needs and develop strategies for improvements; and to support connections and networking between family organizations, care coordinators, providers and parent leaders through CAM and other forums and activities.
CYSHCN program staff continue to provide technical assistance to LHJ CYSHCN coordinators through multiple methods including materials development and live assistance through phone, teleconference, webinar and in-person site visits. We ask participants to evaluate: (1) information and discussion on issues related to CYSHCN; (2) information, discussion and clarity on ICD-10 codes and resources; and (3) information, discussion and clarity of CHIF technical support. Evaluations show high scores for satisfaction with the site visits. We will continue them in FFY 2020 to onboard new CYSHCN coordinators and orient them to the CYSHCN Manual.
The CYSHCN program will continue to provide technical assistance to providers regarding nutrition-related resources, including workforce capacity building and ongoing education through the MCHBG-funded UW nutrition contract. Further capacity-building activities during FFY 2019 and FFY 2020 will be based on results from the FFY 2017-18 Needs Assessment of Nutrition Services for CYSHCN across the state, which will be published in summer 2019.
The CYSHCN program conducted a statewide telehealth capacity assessment of services for children and youth with autism and other developmental disabilities, in partnership with autism stakeholders, as part of ongoing work through the AS3D grant. The assessment included a review of Medicaid coverage, state laws and rules; administration of a provider capacity survey, a family and caregiver survey, and follow-up interviews (in English and Spanish); and key informant interviews with a variety of providers (e.g., psychologists, physicians and behavioral technicians).
The Creating Connections capacity assessment report published in 2017 shares recommendations for expanding existing telehealth infrastructure. Some of those recommendations will be incorporated into AS3D-specific work and some can be applied more broadly through MCHBG work (such as coordinating with our regional Telehealth Resource Center, providing information and technical assistance on the use of telehealth to providers when possible, educating families and consumers about telehealth as an option for care, and to ensure that family choice and voice are included in telehealth efforts).
In December 2018, the Creating Connections Strategic Plan was published, setting a course for building telehealth capacity and use of this technology across the state. Our Public Health Nurse Consultant, who led this project, received multiple invitations to present our telehealth capacity assessment and strategic plan at both in-state and national meetings. The telehealth strategies created through our AS3D grant will continue after the end of the grant in August 2019 and will be supported through cross-agency work to coordinate telehealth supportive activities. Successful expansion will require technical assistance to be available for external partners implementing telehealth in their clinical practice. Telehealth expansion provides an opportunity for more children to get timely access to diagnostic evaluations and support services they need.
Objective CS-4: Policy
Develop, advance and/or implement appropriate policies to support and sustain statewide systems improvements, community supports and resources for CYSHCN (including Genetics and EHDDI) and their families so that they reach their full potential.
Strategy CS-4.1
Explore, pursue and promote possible mechanisms to facilitate and fund components of the medical home model of care, including care coordination and health care transition.
- Explore options to expand care coordination under the Medicaid Health Home model to be available for all CYSHCN, and develop strategies to ensure that it is financially sustainable.
- Encourage primary care practices to adopt medical home practices by promoting reimbursement mechanisms that support the additional functions of a medical home.
- Promote statewide policies for improved early identification of CYSHCN to ensure that these children and youth are referred to appropriate types and sources of enhanced care.
Strategy CS-4.2
Improve data and information sharing among key system partners.
- Update and maintain Title V-Title XIX data sharing agreements and access to client information to promote care coordination for CYSHCN. COMPLETED
- Encourage and advocate for policies that allow for streamlined information sharing between providers, MCOs, and other care coordinators.
- Explore opportunities to facilitate the development and execution of data sharing agreements to reduce barriers between the Health Insurance Portability and Accountability Act (HIPAA), Family Educational Rights and Privacy Act (FERPA), early intervention and social services data sources, which will improve families’ and providers’ abilities to use shared plans of care. COMPLETED
Status to Date and Upcoming Plans for Objective CS-4
The CYSHCN program is updating and expanding the Washington Administrative Code (WAC) to provide additional structure for facilitating the program. The old WAC is out of date and no longer accurately reflects our program or the work it performs. The updates will make the scope much easier to understand.
Adequate Insurance Coverage and Health Care Access for MCH Consumers: A Policy Influence Approach
Our ESMs for National Performance Measure 15 are:
- Title V effort to influence key policies that impact insurance adequacy for Washington CYSHCN
- Title V progress on influencing key policies that impact insurance adequacy for Washington CYSHCN
We track both effort and progress to recognize that some policy changes require years of effort, and that progress toward our goals fluctuates because of many factors, including ever-changing political will of elected officials and voters over time.
We exceeded our 2018 ESM goal of one policy/procedure: we worked on 14 policies and procedures that year. Some examples include providing technical assistance resulting in families getting needed equipment and services for their children, and insurance coverage for those items, as well as providers knowing how to submit claims correctly; and working with HCA and other partners at a systems level to address insurance adequacy-related issues. For 2020, we have set a goal to make an effort to influence at least ten policies, and make progress on at least one policy.
To provide some background, beginning in FFY 2017 Title V staff from multiple programs (“Policy ESM Workgroup”) met to explore alternatives for how to take an evidence-informed approach to policy influence.
We started with the graphic representation of the policy cycle shown below (EcoInformatics International Inc.), which contains the four major phases of policy development: agenda setting, policy formation, policy implementation and policy review.
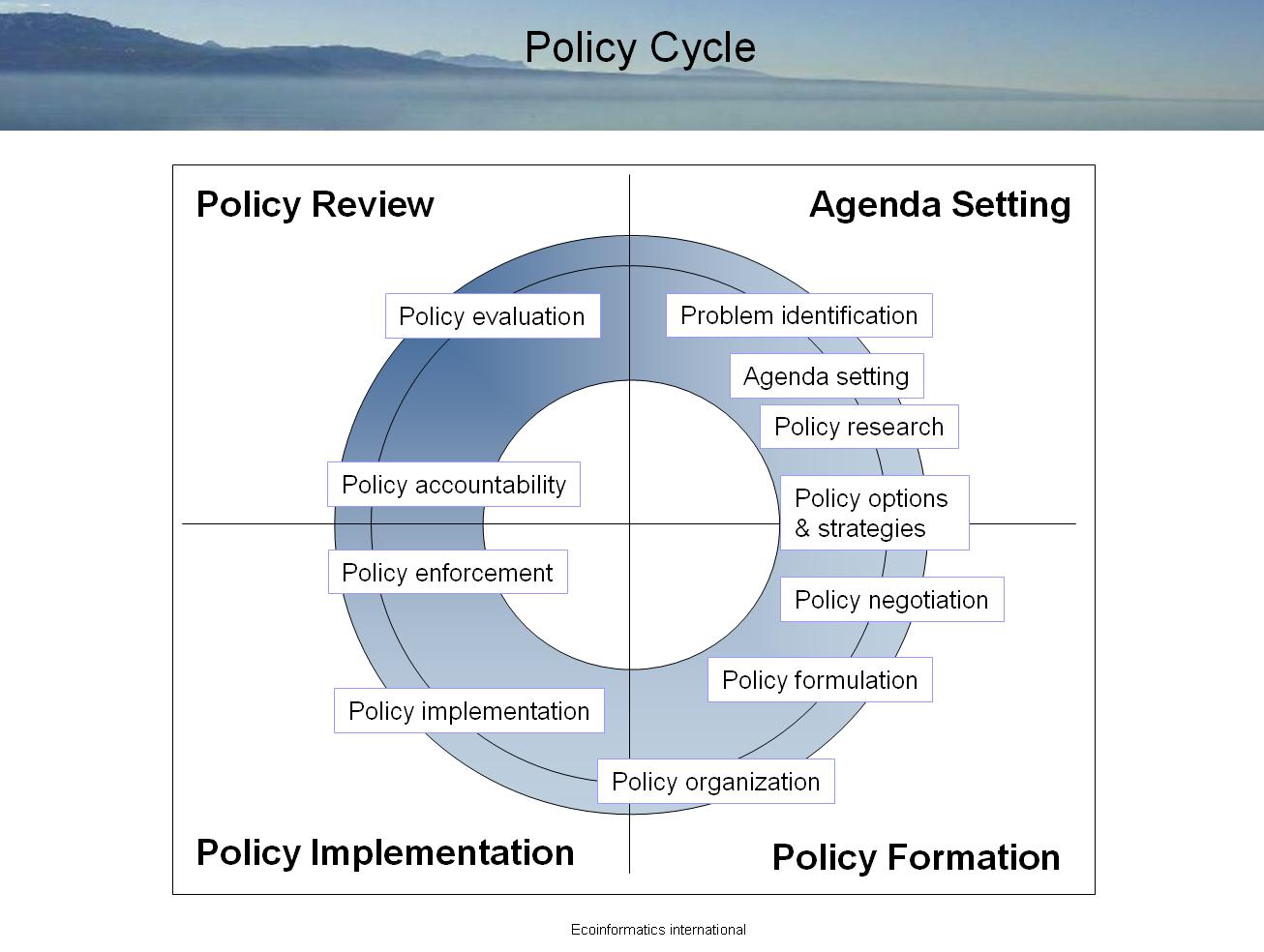{kind=link}

This representation of the policy cycle aligns with major theories of policy development and implementation, including but not limited to Ripley (in McCool, D.C., ed. Public Policy Theories, Models and Concepts, 1995) and Anderson (Anderson, J.E. Public Policymaking 6th ed., 2006).
The Policy ESM Workgroup re-labeled the sub-phases of the policy cycle to reflect how Title V staff attempt to influence policies that are often not under the authority of our programs, but that have significant impacts on the populations we serve. The policy cycle we are using is shown below.

From this, we created a Policy Influence Planning and Tracking Tool with the following elements:
- A description of the policy we are attempting to influence and the changes to that policy that would benefit our focus population(s)
- Which MCH populations are impacted by the policy
- Which levels of the MCH pyramid the policy impacts
- Which entities have decision-making authority over the policy in question
- The role(s) of the Title V program regarding the policy (e.g., convener, educating and informing stakeholders, providing training or technical assistance, assisting with policy review, etc.)
- A list of key stakeholders for the policy
- A table with space for brief descriptions of past activities, current status and plans for progress for each of the 15 sub-phases of the policy cycle
We piloted use of the tool and explored how to derive possible ESMs using the tool with several major policy influence efforts we have underway in the CYSHCN, Perinatal/Infant Health, and Women/Maternal Health domains:
- Medicaid coverage of enteral nutrition for CYSHCN
- Moving neurodevelopmental centers from a fee-for-service to a managed care payment structure
- Updates to state regulations for prenatal diagnosis (to include coverage for certain screenings)
- Changes to Medicaid coverage of postpartum long-acting reversible contraception (LARC)
The workgroup created a tool to quantify measurement of progress (positive change) and effort (work) related to policy development, and will continue to further develop this concept.
Objective CS-5: Adequate Insurance
By September 30, 2020, improve access to adequate public and private health insurance for CYSHCN.
Strategy CS-5.1
Increase Title V/MCH program staff understanding of health reform and health transformation at the state and local levels.
The CYSHCN unit uses Catalyst Center tools to better understand the landscape of health reform and health transformation at the state and local levels; once completed, identified action steps will be pursued and will inform the strategies and activities below. COMPLETED in FFY 2016
Strategy CS-5.2
Promote performance, payment and reimbursement reform.
Work with partners to…
- Identify gaps and issues where current levels of coverage are not meeting the needs of CYSHCN and where co-pays and deductibles place undue burden on families; e.g., underinsurance, incorrect billing of patients, waiting lists, and wait time for eligibility decisions for DSHS and Developmental Disabilities Administration (DDA) programs.
- Advocate for performance or financial incentives to promote medical homes and reimbursement for care coordination to enhance access to services and promote quality.
- Advocate for policies that ensure all children, including CYSHCN, have access to medically necessary services and that those services are delivered in culturally and linguistically appropriate ways.
- Promote systems capacity to assure CYSHCN and their families have geographical, timely and affordable access, with limited out-of-pocket expenses, including high deductibles, to comprehensive community services, resources and supports.
Strategy CS-5.3
Collaborate with key partners to standardize and streamline insurance coverage and access. Identify state-specific activities to blend system principles, standards and measures with the National Standards for Systems of Care for CYSHCN domains that include access to care and insurance and financing.
- Work with partners to improve insurance authorization processes.
- Partner with family-led organizations to standardize and streamline coverage and access, and include funds in contracts with partners to reimburse parents for participation where appropriate.
- Educate HCA on National Standards for Systems of Care for CYSHCN and suggest adding supporting language into the procurement processes for publically-funded managed care contracts. COMPLETED
- Assess adherence to Affordable Care Act (ACA) covered services by the private health insurance plans for non-Medicaid/privately insured CYSHCN, including coverage for hearing screening and developmental screening according to the Bright Futures Guidelines Periodicity Schedule with no cost sharing to parents.
Strategy CS-5.4
Assure maximized implementation of federal and state health reforms as relates to CYSHCN. Participate in interagency efforts to implement the Affordable Care Act, impact Essential Health Benefits and blend physical, mental and behavioral health services into comprehensive health care.
- Explore ways to highlight and address the needs of CYSHCN in the HCA Healthier Washington initiatives, including Accountable Communities of Health and Medicaid transformation.
- Support the UW MHPP in their efforts to track and provide electronic updates about health care reform and transformation in Washington, especially as it relates to medical homes for CYSHCN.
Status to Date and Upcoming Plans for Objective CS-5
Although the ACA has had very positive impacts on health insurance in Washington (a decline in our total uninsured rate, increased access to care for more adults, affordable health coverage for low- and middle-income residents, cost-sharing reductions and a steady growth in insurers and health plans), many CYSHCN in the state still do not have adequate insurance to meet all of their medical needs (63.7 percent, NSCH 2017).
As a result, much of the work that the CYSHCN program staff does in this priority area focuses on influencing policies that impact insurance adequacy for CYSHCN. Though our program, and often DOH as a whole, does not have decision-making authority over many policies that directly impact insurance adequacy for CYSHCN, we often have relationships with the agencies or entities that do have decision-making authority.
MCHBG-funded CYSHCN program staff play a variety of roles in influencing policy decisions, including convening partners; providing technical assistance; educating and informing stakeholders; and assisting decision-makers in reviewing policies, identifying alternate policy solutions, identifying barriers to policy implementation, and implementing and/or facilitating policy implementation. Often these roles allow us to influence policy by helping to set policy agendas (identifying problems and raising awareness of issues, getting buy-in to address the issue, getting ourselves and other key stakeholders such as family leaders a “place at the table” where policies are discussed, and proposing options and strategies). We are sometimes involved in policy formation (discussing and negotiating policy options; choosing policy options; and formulating, constructing and finalizing policies). We are often involved in implementing policies (engaging in policy/program planning; developing formal and informal procedures; promoting, educating and informing those impacted by policies; and identifying and addressing potential and actual barriers to effective policy implementation).
One example of influencing policy within our agency: Many of our external partners have expressed concern that the suicide rate is high among CYSHCN with autism and in the disability community in general. Autism and intellectual and developmental disabilities are not specifically reflected in the language of Washington State’s Suicide Prevention Plan.
CYSHCN program staff consulted with internal staff who conduct the Healthy Youth Survey. The Healthy Youth Survey is a shared data collection effort, led by staff from DOH, staff from our Office of Superintendent of Public Instruction, and DCYF. It includes a data set of disability questions that are rotated on and off the survey, which is completed every two years in 6th, 8th, 10th and 12th grade classrooms around the state. The 2012 survey showed that those who self-reported a disability showed significantly higher thoughts of suicide, plans of suicide, and attempts at suicide. The disability data set was not included in subsequent surveys until 2018 and was not planned again after that. After multiple conversations with DOH staff, they were very supportive about reaching out to partners, and were able to get the other two agencies to commit to including the disability questions in the 2020 survey. This will allow us additional time to identify opportunities for better surveillance for CYSHCN sub-populations at high risk for suicide.
In FFY 2018, the CYSHCN program’s nutritionist provided technical assistance to providers regarding the Washington State Administrative Code enteral and medical nutrition therapy regulations and billing. The CYSHCN program is currently helping to draft a new enteral and medical nutrition therapy WAC.
The CYSHCN program nutritionist retired in May of 2018 but was brought back part-time in December 2018 to support the program, as there was an internal delay in filling the vacant position. She continues to work to support the finalization, publication, and dissemination of the statewide nutrition needs assessment, and will provide assistance to onboard a successor to prevent gaps in priority nutrition work. One goal we would like to work on when this position is filled, is to work with Medicaid to revise the WAC on the coverage of metabolic low protein foods. There is some discrepancy in the language between the Revised Code of Washington and the WAC, which creates a gap in coverage for these vital life-saving food products.
CYSHCN program staff will continue to identify gaps, issues and opportunities to assist families where current levels of coverage are not meeting the needs of CYSHCN. DOH is monitoring the effects of health care reform related to benefits, eligibility and community access to services and identifying gaps. DOH is collecting stories from families to demonstrate impacts. To address gaps in Medicaid, DOH will continue to work with the HCA on leveraging Medicaid resources where appropriate. The CYSHCN program is actively pursuing opportunities to be “at the table” to understand current health care transformation activities. The advancement of value-based reimbursement models is based on the needs and goals of providing care and reducing costs to adults with chronic health conditions. More effort is needed to identify strategies to support children, especially those with clinical medical complexity, to ensure they have access to qualified providers, who are able to receive appropriate reimbursement for the complexity of providing and coordinating their care.
To Top
Narrative Search