


III.C.2.a. Process Description
I. Goals, Framework, Methodology
The goal of the Wyoming Maternal and Child Health Unit’s (WY MCH) Five-Year Needs Assessment (NA) was to determine maternal and child health (MCH) priorities that reflect stakeholder input, are supported by evidence, and which WY MCH has the capacity to address. WY MCH based its NA framework on the six-step Peterson and Alexander NA process and the John M. Bryson strategic planning process. The NA stages are: start-up planning, operational planning, data, needs analysis, program and policy development, and resource allocation. WY MCH adopted core values in 2015 and revised these core values during the start-up planning stage to drive key decision-making during the 18-month process. The core values include:
Data-driven:
WY MCH uses data, evidence, and continuous quality improvement
Engagement:
WY MCH cultivates authentic collaboration and trust with families and community partners
Health Equity:
WY MCH integrates an understanding of how differences in social, economic, cultural, and environmental factors across generations and throughout the lifespan impact health
Life Course Perspective:
WY MCH integrates an understanding of how risk and protective factors influence health across the lifespan and across generations
Systems-Level Approach:
WY MCH prioritizes work that addresses community structures, social norms, environment, and policies to maximize impact
The Start-up Planning Stage began in November 2018 with the establishment of a leadership structure for implementing the NA process. A planning group consisting of internal MCH staff (Title V Director, program managers (PMs), and MCH Epidemiology staff) determined the NA goals, participants, target populations, and timeline and developed a Steering Committee of leaders from WDH, state government, and the community to inform and guide the process and hold the Planning Group accountable to the developed plan.
In the Operational Planning Stage, the Planning Group developed an NA project charter that was approved by the Steering Committee in May 2019. They also developed a stakeholder engagement plan including development of MCH Priority Action Teams (PATs) (whose membership would be further defined after narrowing potential priorities and a survey of state partners), reviewed qualitative data during State Health Assessment (SHA) community meetings, and compiled data from existing state and national sources.
The Data Stage, led by MCH Epidemiology, focused on building a Title V National Outcome Measure (NOM) Tableau dashboard using the Federally Available Document produced by the Health Resources and Services Administration as well as additional state survey data (e.g. National Survey of Children's Health (NSCH), Pregnancy Risk Assessment Monitoring System PRAMS)) and Vital Statistics Services (VSS) data. The SHA community meetings, MCH partner survey data, and MCH PAT meetings provided additional qualitative data on the strengths and needs of the WY MCH populations.
The Needs Analysis Stage occurred in several iterations; in each, the depth of data presented to decision makers increased and the potential priorities decreased. The image below demonstrates the narrowing of potential priorities from all available NOMs to a final list of Title V priorities.

WY MCH staff conducted an initial assessment of each NOM on their perception of its magnitude/burden, MCH leadership role, internal capacity and feasibility, and political leverage. MCH epidemiologists evaluated each indicator for data availability, relation to national indicators, and alignment with themes from the SHA community meeting qualitative data. Following a formal scoring process in May 2019, a narrowed list of NOMs (i.e. “1st Cut”) representing the top two quartiles of scored NOMs within each population domain became potential priorities.
In summer and fall 2019, MCH PMs conducted a feasibility assessment for each potential priority topic to evaluate NOMs and national performance measures (NPMs) in terms of current activities in the state, the role of MCH, the availability of strategies, and current state capacity.
Program staff also completed a Strengths, Weaknesses, Opportunities, and Threats (SWOT) analysis of 2015-2020 NPMs and the narrowed list of potential priority topics for 2021-2025. MCH program managers conducted key informant interviews with stakeholders, reviewed literature on evidence-based strategies, and consulted the MCH Evidence Center to conduct the feasibility assessment. Findings for each priority topic were summarized in a standard NOM overview template with a recommendation and justification for keeping or deleting the priority topic. MCH PMs presented their recommendations to the planning group, then finalized a narrowed list of NOMs for consideration (i.e. “2nd Cut”) and presented it to the Steering Committee for approval in January 2020 and the general public (including MCH PAT members) in February 2020.
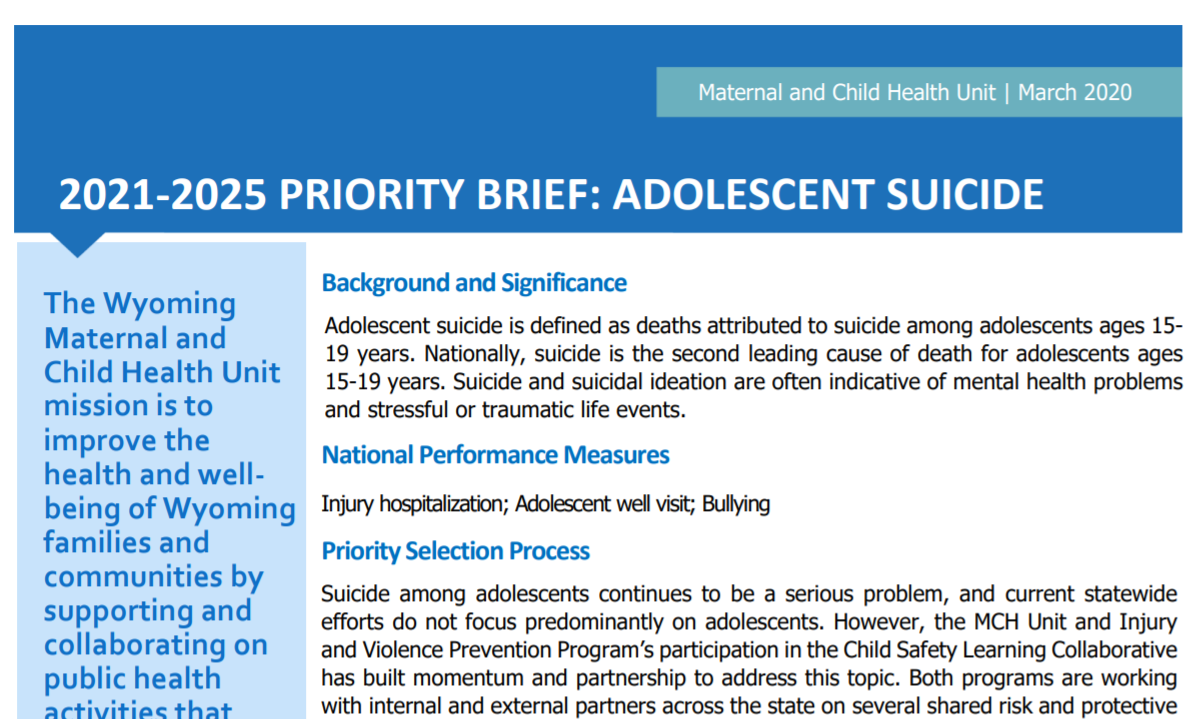
The final step in the Needs Analysis Stage was the development of priority briefs for each potential priority topic for review by stakeholder groups (i.e. MCH PATs) representing each of the potential priority topics. Each priority brief covered the background/significance of the priority topic, associated NPMs, priority selection process summary, key data, and available strategies. An excerpt can be viewed here.
In March 2020, WY MCH convened five MCH PAT meetings, each representing one or two potential priority topics. These meetings marked the beginning of the Program and Policy Development Stage and strategic planning process outlined below, which highlights key internal and external meetings that moved WY MCH from priority selection to strategy selection, measure selection, and the development of a State Action Plan.

The purpose of the March MCH PAT meetings was to share information that informed proposed priority selection and collectively discuss possible strategies for implementation. This convening offered final input on the selection of potential priorities (Needs Analysis Stage) and initial input on the selection of strategies to address each priority topic (Program and Policy Development Stage). The five MCH PAT meetings addressed:
- Systems of care for CYSHCN
- Adolescent suicide
- Maternal and infant mortality
- Child/adolescent mortality with a focus on motor vehicle mortality
- Child obesity/overall child health
At each meeting, the Title V Director provided background on Title V and the NA process to date, followed by brief presentations by the lead WY MCH PM on information contained in their respective priority briefs. Then, a contracted facilitator led an interactive dialogue among participants to reflect on the priority brief information, ask questions, gather input, and offer additional strategies for consideration. A note-taker recorded the dialogue.
Following the MCH PAT meetings, WY MCH distributed a stakeholder survey to gather input on the strategy options discussed and gauge partner capacity to support. Survey results were shared with each WY MCH PM to assist in strategy selection.
PMs completed an MCH Activity Prioritization Tool that weighed various potential activities/strategies among six strategy screen elements and the five MCH Core Values. These scores further support the prioritization of specific strategies for implementation.
Due to COVID-19, WY MCH met virtually for a four-day strategic planning retreat in April 2020 consisting of nine separate, facilitated one- to two-hour sessions. A contracted facilitator launched the retreat with an introduction to strategic planning and an overview of Strategic Doing and Agile Leadership concepts, including using individual and team strengths in planning and implementation. Subsequent sessions focused individually on each priority topic and the proposed strategies to address them based on feedback from the March PAT meetings, PAT follow-up survey results, and the results of the MCH Activity Prioritization Tool. In addition, PMs proposed associated NPMs or state performance measures (SPMs) and draft evidence-based or -informed strategy measures (ESMs).
After the conclusion of the internal strategic planning sessions, WY MCH began the final stage of strategic planning by preparing priority logic models to help visualize the connection between the priority need, investments, strategies, and associated measures. An example logic model is below.

In late May 2020, WY MCH reconvened MCH PATs virtually to present results of the March PAT meeting follow-up survey and MCH Activity Prioritization Tool and a summary of internal strategic planning, and to reveal final draft versions of each priority topic’s logic model. The May PAT meetings successfully engaged stakeholders as evidenced by strong attendance, interactivity and commitment to action, and partnership on the part of the stakeholders.
WY MCH is beginning the final Resource Allocation Stage and will report on its progress within the NA Summary Update submitted in summer 2021.
II. Stakeholder Involvement
As the NA process described above demonstrates, WY MCH involved stakeholders at every stage. Key stakeholder groups and stakeholder engagement methods are described below.
Steering Committee: The Steering Committee involved decision makers (e.g. PHD, WDH, partner organization representatives, Wyoming Medicaid, Wyoming Family Voices) to guide NA development, approve priorities, and hold MCH accountable to the plan. The Steering Committee membership was defined in early 2019 with its first meeting held in May 2019, during which the NA plan and charter were approved. The Steering Committee met in January 2020 to approve draft priorities. The Steering Committee also informed the development and membership of MCH PATs and will approve the final priorities and final State Action Plan prior to October 2020. During the 2021-2025 grant cycle, the Steering Committee will meet once per year to monitor progress on the WY MCH State Action Plan.
SHA Community Meetings: WY MCH aligned with SHA efforts and used results from community meetings held in nine counties to help guide early priority decisions. Counties were selected based on urban, rural, and frontier classification; geographic position; county health rank; and minority populations. The MCH Epidemiology Program evaluated the recorded comments from these community meetings by topic area, and those that aligned with one of the Title V NOMs were placed in that NOM category. Those NOMs with the largest amount of comments overall, about problems or barriers, and about what the community currently does well were highlighted and considered by program staff during initial NOM selection. The summary can be found here.
Stakeholder Newsletters and Webinars: WY MCH used its newsletter platform to formally launch the 2021-2025 NA process in January 2019 by featuring the Title V NA requirements and releasing a brief survey inviting stakeholders to help identify MCH population needs. Subsequent newsletters and two stakeholder webinars held in June 2019 and February 2020 featured NA updates and opportunities for stakeholders to provide input.
Partner Survey: The partner survey distributed in the January 2019 newsletter solicited feedback from stakeholders on challenges facing MCH populations and ranking of available NPMs. The survey was sent to over 400 WDH, state, and community partners and received 37 responses. All respondents reported working across multiple population domains and half worked for the State of Wyoming. Major challenges facing MCH populations included access to care, social determinants of health, and access to resources.
Priority Action Teams: After the first cut of potential priority topics, MCH PATs were developed for each priority topic to inform development and implementation of the 2021-2025 State Action Plan. Members were selected based on expertise, experience, and work related to priority topics. MCH PAT members contributed to the priority selection process by completing the MCH partner survey, participating in key informant interviews during the feasibility assessment, and providing key input on selection of strategies to address state priority needs during two spring 2020 meetings.
Public Input Process: WY MCH released a public input survey summarizing programs’ report and application content. Survey questions addressed alignment between program activities and community needs, barriers, and health equity. WY MCH received 107 responses from 21 of Wyoming’s 23 counties and utilized this feedback to finalize strategies and identify new community partners and local support for selected priorities.
III. Quantitative and Qualitative Methods
WY MCH and the MCH Epidemiology team used a variety of methods to assess the strengths and needs of each of the six domains. Quantitative methods included analyzing Wyoming-specific NOMs in comparison to the U.S. Where possible, these measures were broken down and examined by different populations (e.g. age, gender, race, ethnicity, socioeconomic status) to better understand disparities. Qualitatively, the Wyoming SHA was utilized. Responses/comments from members of the community that mentioned MCH populations were evaluated.
IV. Data Sources
Data from many different sources were utilized to inform the NA process. Quantitative analysis relied on the Federal Available Document (FAD) produced by HRSA to examine both NOM and NPM data. Data from surveys (e.g. NSCH, PRAMS) and Wyoming VSS data was utilized, outside of what was already provided in the FAD, to further look at disparities facing MCH populations. Qualitative data from the SHA Community Meetings was utilized to assess perceptions of needs and successes related to health broadly as well as those comments specific to MCH populations.
II.C.2.b Findings
III.C.2.b.i MCH Population Health Status
Women’s/Maternal Health
Maternal Mortality and Morbidity
Due to Wyoming’s small population and small numbers of maternal deaths, maternal death rates fluctuate. Aggregated data suggests that the 2013-2017 Wyoming maternal mortality rate is similar to the national rate. An analysis of Wyoming pregnancy-associated deaths from 2013-2015 vital records mortality files indicated 58% of the deaths were classified as accidental, with half due to overdose and half due to motor vehicle crashes. Suicide accounted for 16% of the pregnancy-associated deaths during that time. A joint UT-WY Maternal Mortality Review is currently being implemented to improve understanding of the causes of maternal deaths and surveillance of maternal mortality in Wyoming.
In 2017, Wyoming’s severe maternal morbidity rate of 46.3/10,000 delivery hospitalizations was lower than the rate of 73.1/10,000 delivery hospitalizations the previous year, and significantly lower than the 2017 U.S. rate of 70.9/10,000 delivery hospitalizations (Healthcare Cost and Utilization Project - State Inpatient Database). Comparisons to the rate before the implementation of ICD-10 are not possible. The most common severe maternal morbidity in Wyoming is transfusion, followed by eclampsia.
Maternal Mental Health
As suicide and drug overdoses are among the leading causes of maternal mortality in Wyoming, maternal mental health is an area of focus. Wyoming Pregnancy Risk Assessment Monitoring System (PRAMS) continues to collect data on opioid use before and during pregnancy for a second year to have sufficient data to track potential trends and associations between maternal mental health and opioid use. Seventeen point three percent of women reported depression prior to pregnancy, and 15.9% reported depression during pregnancy (PRAMS, 2016-2018).
In Wyoming, the prevalence of postpartum depression (13.2%) is similar to the U.S. rate. Women ages 15-19 reported the highest prevalence of postpartum depression (23.6%), followed by 20-24 years old (19.0%). Reported prevalence of postpartum depression was also significantly higher for women reporting incomes levels ≤100% of the Federal Poverty level (FPL) (17.9%) and 101-200% FPL (16.1%) compared to women reporting incomes ≥300% FPL (6.5%). A majority (84.7%) of women reported their providers discussed depression with them at a postpartum visit, but this did not vary by maternal age group or income level (PRAMS, 2016-2018). Due to small numbers of respondents, differences in reported rates of postpartum depression or providers asking about postpartum depression by race could not be evaluated.
Preconception Health
According to the Behavioral Risk Factor Surveillance System (BRFSS), in 2018 64.8% of Wyoming women reported having a preventive medical visit in the past year, significantly less than the U.S. rate of 73.6% for the same year. These rates were lowest for Wyoming women ages 25-34 years (58.3%) and uninsured women (52.4%). However, due to small numbers, caution should be taken when drawing conclusions in regard to differences in preventive medical visits between different groups of Wyoming women.
PRAMS data (2016-2018) indicate that 4.4% of women had hypertension before their most recent pregnancy and 3.9% had diabetes. During pregnancy, 11.3% of women reported having hypertension and 6.5% reported developing gestational diabetes. Several PRAMS respondents commented on the barriers to high-risk maternal care in their community.
Maternal Smoking
National Vital Statistics System (NVSS) data show significant reductions in the percent of women giving birth reporting smoking during pregnancy since 2009, both in Wyoming and the U.S. In 2018, 13.4% of Wyoming women giving birth reported smoking during pregnancy, compared to 19.3% in 2009. Wyoming PRAMS data also indicate reductions in smoking during the last three months of pregnancy.
Family Planning
In 2018, 26.1% of women reported having an unintended pregnancy, down slightly from 2012 when 33.1% percent of women reported having an unintended pregnancy; this is not a significant change. In 2018, 16.7% of women reported being unsure of what they wanted in regard to being pregnant and this has stayed consistent since 2012 (PRAMS). The rate of unintended pregnancies did not differ by race, but differences were seen by income level. Women with reported incomes of ≤100% FPL reported having an unintended pregnancy significantly more (40.0%, 95%C CI:34.8%-45.5%) than women with incomes greater than >100% FPL.
In 2018, 34.4% of Wyoming women reported use of the most effective form of contraception (including permanent methods and highly effective reversible methods). This dropped slightly from 2017 (29.8%) but has not changed significantly since 2012. In 2018, 25.4% of women reported the use of moderately effective birth control, and this has not changed significantly since 2012.
Perinatal/Infant Health
Infant Mortality
Wyoming’s 2014-2018 infant mortality rate (IMR) was 5.2 deaths/1,000 live births, with 33.3% of the deaths occurring among postneonatal infants and 66.7% among neonatal infants. The Wyoming IMR was lower than the national rate of 5.8 deaths/1,000 live births in 2017 and meets the Healthy People 2020 (HP2020) objective (6.0 deaths/1,000 live births). Both the neonatal and postneonatal mortality rates have been similar to U.S. rates. The leading causes of deaths for neonatal infants were congenital malformation, deformations, and chromosomal abnormalities, followed by disorders related to short gestation and low birth weight. For postneonatal infant deaths from 2014-2018, the leading causes were sleep-related sudden unexpected infant death (SUID), followed by congenital malformation, deformations, and chromosomal abnormalities (Vital Statistics Services (VSS)).
Due to small numbers, differences in IMR by subpopulation are difficult to ascertain. VSS data indicate that Wyoming's neonatal IMR is significantly higher than the U.S. for those reporting a public insurance other than Medicaid, which is not observed in the postneonatal IMR. Disparities by county in infant mortality from 2009 to 2018 are also seen, ranging from 3.2 deaths/1,000 live births in Teton County to 8.6/1,000 in Goshen County, indicating the need for further exploration in potential existing disparities across the state. From 2015 to 2017, the IMR was significantly higher among infants born to women with less than a high school education (11.1/1000), compared to some college (4.0/1000) or those with a college degree or higher (2.7/1000). A noted gap in services is that Wyoming has no Level III NICU facility.
Preterm and Low Birthweight Births
Between 2009 and 2018, the prevalence of low birthweight and preterm deliveries in Wyoming, which are leading causes of death among neonatal infants, remained relatively stable. These did not differ much from the U.S. prevalences. In 2018, Wyoming had not met the HP2020 preterm goal of 9.4%, with 9.8% of Wyoming births being preterm, or the HP2020 low birthweight goal of 7.8%, with 9.4% of Wyoming births being low birthweight (VSS, 2018).
In 2018, Wyoming saw significantly higher prevalences of premature and low birthweight births for women giving birth who are uninsured compared to the U.S. rate (VSS). Women under 20 years of age giving birth had the highest prevalence of preterm and low birthweight births (13.2% and 13.4%), with the low birthweight prevalence significantly higher than for women ages 25-29 and 30-34 giving birth. A promising observation for Wyoming in both 2017 and 2018 was that the prevalence of very low-weight births in Wyoming (0.9% and 1.1%) was significantly less than the prevalence of very low birthweight births in the U.S. (1.4% and 1.4%) (VSS).
Infant Sleep Environment
As mentioned, a leading cause of death among postneonatal infants in Wyoming is SUID, which includes sudden infant death syndrome (SIDS), accidental suffocation and strangulation in bed, and unknown causes. SUID accounted for 37.4% of postneonatal deaths in Wyoming from 2009 to 2013 and 41.8% of postneonatal deaths from 2014 to 2018. Eighty-five point five percent of Wyoming women reported their infants are put to sleep on their backs (PRAMS, 2016-2018), exceeding the HP2020 goal of 75.8%. This did not differ between women of different races, ages, or income levels.
During this same time period, 76.8% of women reported their infants always or often slept alone in their crib or bed. This differed by maternal age, with 15-19-year-olds reporting this significantly less often (55.1%) compared to 24-34-year-olds (80.0%) and those women 35 years of age or older (78.2%). American Indian women reported their infant always or often slept alone (66.2%) significantly less than White women (79.4%). Differences by income level were also observed, with women reporting incomes >300% FPL also reporting that their infant slept alone always or often (86.7%) significantly more than women reporting incomes 0-100% FPL (70.7%) and 101-200% FPL (73.4%) (PRAMS, 2016-2018).
Additional disparities in infant sleep environments were also seen by race/ethnicity and income level. American Indian women reported significantly more often that their infant slept on a twin mattress or bed (50.8%) compared to white women (24.0%), and significantly less often that their infant slept in a crib, bassinet, or Pack & Play (76.8%) compared to White women (89.5%). Women reporting incomes ≥301%FPL reported their baby sleeps in a crib, bassinet, or Pack & Play significantly more (94.1%) than women reporting incomes of 0-100% FPL or 101-200% FPL (80.9% and 85.1%). Women reporting higher incomes were also reporting significantly less that their baby slept with a blanket (53.7%) compared to women reporting incomes 0-100% FPL (74.7%) or with toys, a cushion, or a pillow (5.5%) compared to women reporting incomes 101-200% FPL (13.2%).
A noted gap seen is that while American Indian women reported a health care provider spoke with them about placing their infant to sleep in a crib, bassinet, or Pack & Play (85.2%), placing a crib in the same room as them (58.5%), and what things should and should not go in bed with their infant (86.4%) significantly more often compared to White women (76.4%, 43.5%, and 77.1%), this is not reflected in the actual sleep environments for infants as reported and noted above. There was no difference seen in provider counseling on safe sleep environments by income level, indicating disparities around barriers to providing a safe sleep environment potentially exist more between different socioeconomic statuses, which potentially could be better addressed.
Breastfeeding
Previous MCH work in Wyoming had been focused on improving breastfeeding initiation and duration. Breastfeeding initiation rates in Wyoming continue to exceed (90.6%) the HP2020 Goal of 81.9% children who are ever breastfed (PRAMS, 2016-2018). No difference is seen by maternal age; however, disparities are observed by education level, with women with >12 years of education being significantly more likely to initiate breastfeeding (93.3%) than both those with 12 years of education (86.8%) and with <12 years of education (83.2%). Disparities in regard to breastfeeding initiation are also observed by race, with White (92.2%) and Hispanic (95.5%) women reporting initiating breastfeeding significantly more than women who are American Indian (76.9%) or other races (73.3%) in Wyoming (PRAMS, 2016-2018).
Wyoming also exceeded (31.4%) the HP2020 Goal of 25.5% of children who are breastfeed exclusively through six months (National Immunization Survey, 2016).
Child Health
Child Mortality
In 2018 the Wyoming mortality rate for children ages 1-9 (CMR) was 17.0/100,000. The CMR has remained fairly constant since 2009 and has not significantly differed from the U.S CMR. NVSS data from 2016 to 2018 reveals a gender difference in the CMR, but Wyoming data indicate no significant difference in the CMR between males (17.9/100,000) and females (20.0/100,000) during the same time period (NVSS).
Unintentional Injury
Unintentional injury remains the second-leading cause of death (after natural causes) for children ages 1-9 in Wyoming, and rates are significantly higher than the U.S. rates. From 2008 to 2018, 24% of injury deaths among 1-4-year-olds and 26% among 5-9-year-olds in Wyoming were due to motor vehicle traffic causes, the leading contributor to injury deaths in both age groups (VSS).
Because of Wyoming’s small population and small number of childhood deaths, data on childhood injury outside of fatalities is vital to informing programmatic efforts. WY MCH relies on state hospitalization and outpatient discharge data for non-fatal injury information. There are challenges in collecting accurate and consistent non-fatal injury data. In addition, the switch from ICD-9 to ICD-10 in Wyoming hospitals led to difficulty in classifying injury hospitalizations.
According to the HCUP-SID, the Wyoming child injury hospitalization rates in 2016 (88.0/100,000) and 2017 (119.9/100,000) were both lower than the U.S. rates, significantly so in 2016. The increase seen in Wyoming between 2016 and 2017 was not significant.
Overall Health and Preventative Care
Most children ages 0-11 years (92.6%) were reported to be in excellent or very good health, 48.9% received care in a medical home, 61.9% had adequate and continuous insurance, and 22.4% received care in a well-functioning system (NSCH). Data indicate that children with a medical home were reported as being in excellent or very good overall health significantly more compared to those children who did not have a medical home.
Wyoming parents reported that 22.5% of Wyoming children 9-35 months old received a developmental screening using a parent-completed screening tool in the past year (NSCH, 2017-2018), down from 27.0% the previous two years combined (NCSH 2016-2017). In 2018, 64.2% of eligible, Medicaid-enrolled children ages 1-9 who should receive at least one initial or periodic Early and Periodic Screening, Diagnosis and Treatment (EPSDT) screening received at least one such screening. The percent of eligible children receiving at least one EPSDT screening in Wyoming has increased by 17.2% since 2013 (Wyoming Centers for Medicare and Medicaid Services 416 report).
Obesity and Physical Activity
In 2016, Women, Infants, and Children (WIC) data indicated that 9.1% of Wyoming children ages 2-4 were obese, with BMIs at or above the 95th percentile, a rate that has been significantly less than the U.S. rate since 2008. Between 2017 and 2018, 13.1% of Wyoming children ages 10-13 were reported as being obese, with BMI at or above the 95th percentile (NSCH).
According to parent reports, 30.2% of Wyoming children ages 6-11 were active for 60 minutes every day, similar to the U.S. rate (NSCH, 2017-2018). Due to small numbers, any noted disparities in physical activity based on special health care needs, race, or ethnicity were not observed. A greater percentage of males of this age group were reported to be physically active for 60 minutes every day (31.4%) compared to females (28.9%); however, this was not statistically different and follows a similar pattern seen in the U.S.
WY MCH has recently developed a Healthy Policies Toolkit to improve overall childhood health in Wyoming, especially around obesity and physical activity. Planned strategies include increasing implementation of the toolkit in schools and organizations.
Adolescent Health
Adolescent Mortality
The Wyoming adolescent (ages 10-19) mortality rate (AMR) has decreased significantly since 2009. In 2018, the Wyoming AMR was 31.8/100,000, compared to the U.S. rate of 32.2/100,000 (VSS). While the adolescent motor vehicle mortality rate (AMVMR) in Wyoming has been decreasing since 2009, it has continued to be significantly higher than the U.S. rate. Unlike the U.S., there was no significant difference in the AMVMR between males in females, at 19.9/100,000 and 20.5/100,000, between 2014 and 2018.
Suicide, Self-Harm, and Risk and Protective Factors
Over the last decade, Wyoming adolescent suicide rates have been increasing at a rate of more than double the U.S. rate, and it was about triple the U.S. rate between 2013 and 2015. For adolescents ages 10-19, suicide made up just under one third (29.8%) of all deaths for this age group from 2008 to 2018 (VSS). Data indicate adolescent males in Wyoming die by suicide at significantly higher rates than females, a trend that is also observed in the U.S. overall. However, due to small numbers in Wyoming, this should be interpreted with caution and disparities by race/ethnicity are difficult to examine. The leading mechanisms for death by suicide for adolescents were firearm and suffocation.
Regarding self-harm in Wyoming, 2009-2016 inpatient hospital discharge data indicated female adolescents ages 12-24 have significantly higher rates of self-harm (74.7/100,000) than males (34.1/100,000), with the leading mechanisms being poisoning and cutting (Wyoming Hospital Discharge Data). According to the Wyoming Prevention Needs Assessment (WYPNA), in 2018 18.5% of students reported ever seriously considering attempting suicide in the past 12 months, compared to 15.3% in 2012.
Bullying is considered a major public health problem, as victims of bullying tend to report more negative feelings such as depression, anxiety, and suicidal ideation. Via parent report, significantly more Wyoming adolescents ages 12-17 were bullied by others (59.6%) compared to in the U.S. (38.9%), and significantly more Wyoming adolescents bullied others (25.0%) compared to 15.3% in the U.S. (NSCH, 2018). In 2018, 32.0% of Wyoming students reported being bullied in the last 12 months (WYPNA, 2018).
Teen Births
Since 2009, the Wyoming teen birth rate (TBR) has significantly decreased like the U.S. rate; however, it continues to be significantly higher than the U.S. rate. The most recent data from Wyoming VSS indicated the 2019 Wyoming TBR was 19.4/1000 females ages 15-19, which is less than half of the rate observed in 2009 (43.4/1000). Differences in rates between races and by county continue to be observed in Wyoming, with American Indian teens having a significantly higher teen birth rate than White and Black teens over the last ten years (VSS).
Overall Health and Preventative Care
For adolescents ages 12-17, significantly fewer (56.1%) were reported by their parents as having adequate and continuous insurance coverage for the entire past 12 months compared to 64.0% in the U.S., and 41.7% of Wyoming adolescents had a medical home. Over half of Wyoming adolescents (54.8%) have experienced at least one adverse childhood experience (ACE), with 33.2% being reported as having experienced two or more ACEs (NSCH, 2017-2018).
In Wyoming 18.1% of adolescents were reported as being physically active for at least 60 minutes every day, with 10.2% being obese. However, the obesity prevalence should be interpreted with caution due to small sample size. Of adolescents ages 12-17, 87.4% were reported as being in excellent or very good health, similar to the U.S. prevalence of 87.2% (NSCH, 2017-2018).
Substance Use
The prevalence of cigarette use among Wyoming adolescents has been decreasing since 2001. In 2001, 16.6% of middle school and high school students reported some cigarette use in the past 20 days. By 2018, this dropped to 6.4% (WYPNA). In 2018 17.2% of high school students and 3.7% of middle school students reported marijuana use at least once in the last 30 days (WYPNA, 2018).
In 2018, 33.7% of Wyoming high school students reported at least one occasion of alcohol use in the past 30 days, down from 44.8% in 2001. Nine point four percent of middle school students reported at least one occasion of alcohol use in the past 30 days, compared to 12.8% in 2001 (WYPNA).
In 2018, 71.3% of Wyoming students reported they perceived using cigarettes once or twice a week to be a great risk of harm. Almost half (45.5%) of Wyoming middle and high school students reported their perceived harm of alcohol use once or twice a week to be a great risk of harm. Of middle school students, 53.0% reported they perceived marijuana use to be a great risk of harm, while only 23.3% of high school students perceived the harm of marijuana use to be a great risk, and 28.7% of high school students reported they thought there was no risk of harm from marijuana use once or twice a week. Half (53.8%) of Wyoming adolescents reported they had spoken with at least one parent about the danger of tobacco, alcohol, or drug use in the past 12 months (WYPNA, 2018).
A challenge faced by WY MCH is that Wyoming no longer administers the Youth Risk Behavior Surveillance System (YRBSS) and the last available year of data in Wyoming is 2015. As a result, infrastructure and capacity for data surveillance among the adolescent population is lessened and making comparisons between Wyoming, other states, and the U.S. is a challenge. Wyoming has worked to identify data sources and systems that will fill the gaps in monitoring the health and wellness of the adolescent population left after the loss of this data source.
Children with Special Health Care Needs (CSHCN)
In Wyoming, 26,977 or 19.4% of children ages 0-17 have a special health care need. Significantly more male (25.5%) than female (13.3%) children have a special health care need, and the prevalence is highest among children ages 12-17 (31.4%). The prevalence of Wyoming CSHCN reported as receiving care in a well-functioning system is 9.7%, compared to 13.9% of CSHCN in the U.S., and a decrease from 16.6% from 2016 to 2017 (NSCH).
WY MCH Children's Special Health Program (CSH) provides gap-filling financial assistance and serves about 640 CSHCH a year, reaching 3.4% of the Wyoming CSHCN population (MCH Program Data, 2018). In 2021-2025, CSH will focus on systems of care in order to reach more of the Wyoming CHSCN population. CSH has recently implemented a genetics telehealth project and a transition to adulthood assessment. In Wyoming, a smaller proportion of CSHCN (13.4%) were reported to have received the services necessary to transition to adulthood compared to the non-CSHCN population (20.3%); in the U.S., a significantly larger proportion of CSHCN are reported to receive the necessary services to transition to adulthood compared to the non-CSCHN (18.9% and 14.2%) (NSCH, 2017-2018).
During 2017-2018, insurance was considered inadequate for a child’s health needs (i.e. it was not adequate or continuous in the past 12 months) for 42.6% of Wyoming CSHCN ages 0-17. Between 2017 and 2018, 38.1% of Wyoming CSHCN were reported as having a medical home, compared to 48.6% of non-CSHCH and 42.7% of CSHCN in the U.S. CSH has identified a need to focus more on the care-coordination component of medical home for the CSHCN population. Similar to U.S. trends, a significantly lower proportion of CSHCN in Wyoming (50.9%) received needed care coordination, compared to 72.8% of non-CSHCN, who needed care coordination.
Additional disparities in health status measures between CSHCN and non-CSHCN status are also observed in regard to physical activity and obesity in Wyoming. A smaller proportion of CSHCN (17.7%) than non-CSHCN (26.4%) are reported to exercise at least 60 minutes every day, and a larger proportion of CSHCN (20.0%) are reported to be obese compared to non-CSHCN (8.6%). Significantly more parents of CSHCN reported concern that their child’s weight was too high (61.1%) compared to parents of non-CSHCN (4.0%) in Wyoming (NSCH, 2017-2018). As a noted priority of promoting physical activity in children via the Child Health domain, a strength of WY MCH is its ability to incorporate CSHCN into other priorities.
III.C.2.b.ii. Title V Program Capacity
III.C.2.b.ii.a. Organizational Structure
WY MCH is housed within the Community Health Section and Public Health Division (PHD) at the Wyoming Department of Health (WDH), which is one of 47 state agencies comprising the executive branch under the leadership of Governor Mark Gordon. PHD is one of four divisions within WDH, joining the Aging, Behavioral Health, and Health Care Financing (i.e. Wyoming Medicaid) Divisions. Within PHD, there are three sections that oversee public health functions and programming. The Community Health Section optimizes quality of life through the promotion of health, protection of community health, and prevention of disease and injury. The other two sections are Health Readiness & Response and Public Health Sciences. Organizational charts for WDH and PHD are attached.
WY MCH and MCH Epidemiology Program staff are funded by federal (including Title V) and State funds that are included in the Title V Maintenance of Effort (MOE). WY MCH also receives the PRAMS, State Systems Development Initiative (SSDI), Rape Prevention and Education (RPE), and Personal Responsibility Education Program (PREP) grants, which provide additional funding for staff and specific programs. MCH block grant funding supports contracts and services to accomplish goals and objectives within each of the five MCH population domains. In addition to funding programs within WY MCH and MCH Epidemiology, Title V funds help build staff capacity in the Injury and Violence Prevention Program. Indirect funds help assure Title V staff have direct access to and support from a Fiscal Manager assigned to WDH-PHD.
III.C.2.b.ii.b. Agency Capacity
Capacity to Provide and Assure Services within Six MCH Domains
WY MCH manages the Title V MCH Services Block Grant (BG) and provides leadership for state and local efforts that improve the health of the MCH population. WY MCH employs nine full-time staff, including a Title V/CSHCN Director, Grants & Contracts Specialist/Title BG Coordinator, four Benefits and Eligibility Specialists, and three Program Managers, each focused on a specific MCH population domain(s). WY MCH programs include Women and Infant Health, Child Health, Youth and Young Adult Health, Newborn Screening and Genetics, and Children's Special Health. WY MCH also partners with the Public Health Nursing (PHN) Unit to implement a statewide home visiting program.
State funding (i.e. MOE/match funds) are allocated via formula to each of Wyoming’s 23 local PHN offices to support local MCH programming.
CSHCN Capacity
Title V funding supports three positions that determine eligibility for the Children’s Special Health Program (CSH), which sits within WY MCH, and provide state-level care coordination services in partnership with local PHN care coordinators. State general funds provide gap-filling financial assistance for families of children that qualify financially and medically for the program. WY MCH contracts with the University of Utah to provide in-person and telehealth (follow-up) genetics clinics annually and genetics consultation to Wyoming physicians.
CSH partners with organizations such as the Wyoming Institute for Disabilities, Uplift, Early Intervention and Education programs, and Wyoming Medicaid, among others, to assure CSHCN and their families receive comprehensive, community-based, and family-centered care. In 2021-2025, WY MCH will work to assess and strengthen the system of care for CSHCN by using the National Standards of Care for CSHCN and developing a CSHCN advisory council.
Since 2012, CSH has lacked direct leadership with the Title V Director overseeing the program and three separate staff members each supervising a member of the CSH team. This structure led to confusion and inefficiencies and diluted the significant importance of this program for WY’s Title V program. To strengthen leadership capacity for CSHCN services in Wyoming, the Title V Director temporarily reassigned the Child Health Program Manager to fulfill current duties as well as interim duties as the CSH Program Manager. Plans are in motion to reclassify a position in 2020 to create dedicated leadership for the CSHCN population domain.
III.C.2.b.ii.c. MCH Workforce Capacity
State Title V program capacity to implement the core public health functions is assessed routinely through efforts of the WDH-PHD Workforce Development Workgroup. A PHD Workforce Training Assessment is completed every two years; the tool assesses workforce capacity using the Core Competencies for Public Health Professionals framework. Assessment results from 2018 are shown below and plans are underway to repeat the assessment in late 2020.


The Capacity Assessment for Title V programs was used as a resource for program staff when completing the Needs Analysis stage of the NA, specifically when interviewing key stakeholders to understand current activities, capacity, and opportunity for partnership for each potential priority topic. The tool may be important to consider completing formally as part of the WY MCH sixth domain priority, “Strengthen MCH Workforce Capacity to Operationalize MCH Core Values.” A University of Wyoming School of Social Work intern placed with the unit for the 2020-2021 school year will assist the Title V Director and staff in developing a comprehensive workforce development plan for MCH staff and contractors.
WY MCH staff are encouraged to use the MCH Navigator platform, which offers a self-assessment and user-directed professional development options to address learning needs at a variety of paces and intensities. While many staff members use the tool, there is no formal requirement and no formal MCH orientation for new staff. This gap represents a significant workforce opportunity leading us into the 2021-2025 grant cycle and one that will be addressed in the sixth domain.
The table below outlines key WYMCH and MCH Epidemiology staff who work on behalf of the Title V program. Brief qualifications are noted for each staff person fulfilling a leadership or management role.
|
Staff Member |
Title/Role |
Unit/ Program |
FTE |
Title V Domain |
Tenure with WY MCH/ MCH Epi (Tenure with State of Wyoming) |
|
Danielle Marks, MSW, MPH |
MCH Unit Manager, Title V Director, and CSHCN Director |
MCH |
1 |
All |
6 (6) |
|
Jamin Johnson, MS, CHES |
Child Health Program Manager and Interim CSHCN Program Manager |
MCH |
1 |
Child; Cross-Cutting |
2 (4) |
|
Rachel Barber, MS |
Youth and Young Adult Health Program Manager |
MCH |
1 |
Adolescent; Cross-Cutting |
2 (2) |
|
Eighmey Zeeck, MPH |
Women and Infant Health Program Manager |
MCH |
1 |
Women/Maternal; Perinatal/Infant; Cross-Cutting |
1 (1) |
|
Sapphire Heien, BA |
MCH Grants and Contracts Specialist, Title V BG Coordinator |
MCH |
1 |
All |
<1 (5) |
|
Carleigh Soule, MS |
Newborn Screening and Genetics Coordinator |
MCH |
1 |
Perinatal/Infant; CSHCN; Cross-Cutting |
14 (14) |
|
Paula Ray |
Children’s Special Health Benefits and Eligibility Specialist |
MCH |
1 |
CSHCN; Cross-Cutting |
20 (20) |
|
Denise Robinson |
Children’s Special Health Benefits and Eligibility Specialist |
MCH |
1 |
CSHCN; Cross-Cutting |
<1 (13) |
|
Sheli Gonzales |
Children’s Special Health Benefits and Eligibility Specialist |
MCH |
1 |
CSHCN; Cross-Cutting |
14 (18) |
|
Ashley Busacker, PhD |
Senior Epidemiology Advisor |
MCH Epi |
1 |
All |
10 (10) |
|
Moira Lewis, MPH |
MCH Epidemiology Program Manager |
MCH Epi |
1 |
All |
1 (1) |
|
Vacant |
PRAMS Coordinator/MCH Epidemiologist |
MCH Epi |
1 |
All |
N/A |
|
Vacant |
MCH/Injury Epidemiologist |
MCH Epi |
.5 |
All |
N/A |
Title V matching funds fully or partially support an estimated 47 FTEs across 23 county PHN offices. The map below demonstrates the total FTEs and MCH population (defined as number of children age 0-19 and number of women of reproductive age (age 20-44).

WY MCH does not currently employ a parent/family member. Wyoming Family Voices identifies a staff member annually to serve as the Wyoming Family Delegate at the Association of Maternal and Child Health Programs. In 2019, WY MCH began convening a monthly parent/family engagement workgroup to discuss and implement collaboration opportunities amongst agencies and programs. In 2020, WY MCH plans to formalize a partnership with the Wyoming Family Voices affiliate through a contract.
During the 2021-2025 NA process, WY MCH identified an emerging, cross-cutting need related to workforce development, both internal and external to the Title V program, due to significant staff transition and retirements. At full staff capacity, WY MCH and MCH Epidemiology represent 13 FTEs. As of July 2020, two MCH Epidemiology positions are vacant. Of the filled positions, over 50% of staff have been in their positions less than three years. Additionally, all staff in management positions have been in their roles less than four years.
During FFY20, WY MCH will experience two retirements of staff members totaling sixty years of collective experience in MCH and service to the State of Wyoming. This loss of experience and institutional knowledge is significant and will require innovation and strong leadership to overcome.
A 2018 assessment of unit activities related to perceived importance of MCH core values further emphasized a need to invest resources and programming to strengthen WY MCH’s ability to operationalize its core values. Staff reported engagement, data-driven, and health equity as the most important core values to communicate to stakeholders. Assessment results indicated opportunities to improve the degree to which all core values drive programmatic decision-making.
III.C.2.b.iii. Title V Program Partnerships, Collaboration, and Coordination
WY MCH partners with MCH Epidemiology for epidemiology and evaluation support for MCH programming. WY MCH also partners with other State agencies and programs to improve MCH population health, including: Health Care Financing (Medicaid and KidCare CHIP); Department of Workforce Services (Early Head Start); Department of Family Services (Child Care Licensing, Temporary Assistance for Needy Families); Department of Education; WDH Behavioral Health Division (Early Intervention, Behavioral Health Treatment, Early Hearing Detection Intervention Program); WDH PHD (Health Readiness and Response, Substance Abuse Prevention, Tobacco Prevention, Injury and Violence Prevention, Chronic Disease Prevention, Immunizations, WIC, PHN); University of Wyoming (Wyoming Institute for Disabilities, School of Nursing, School of Social Work); the Title X grant, administered by an in-state non-profit partner; the federal Maternal, Infant, Early Childhood Home Visiting (MIECHV) grant, administered by an out-of-state non-profit partner; and other statewide organizations and associations (Wyoming Medical Society, Wyoming Primary Care Association, Wyoming American Academy of Pediatrics Chapter, Wyoming American College of Obstetricians and Gynecologists Chapter, Wyoming Kids First, Wyoming Community Foundation).
In 2019, WY MCH, in close partnership with the WDH-PHD Performance Improvement Manager, Rural and Frontier Health Unit Manager, and a Master of Social Work intern, surveyed partners about NA requirements in order to identify collaboration opportunities. Forty-seven percent of respondents responded that their organization had NA requirements. Due to overwhelming interest by partners, WY MCH helped establish a crosswalk of NA requirements including Title V, MIECHV, Mental Health and Substance Abuse Block Grant, State Primary Care Office, Child Abuse Prevention and Treatment Act (CAPTA), Head Start community-wide NAs, SHA, and hospital community health NAs. Efforts to coordinate future NAs continue with the support of an AmeriCorps Vista member assigned to the Performance Improvement Program.
Other Maternal and Child Health Bureau Investments
WY MCH dedicated significant effort in FFY20 to enhance partnership with the Wyoming Family to Family Health Information Center (F2FHIC) and other organizations whose missions include parent/family engagement for MCH populations (e.g. Wyoming Family Voices, Wyoming Parent Information Center, Wyoming Department of Education). Specifically, WY MCH partnered with WY F2FHIC and the Wyoming Institute for Disabilities to coordinate the Title V and F2FHIC NAs. A parent/family engagement workgroup including the partners listed above continues to meet monthly to identify collaboration opportunities.
WY MCH participates in the Mountain States Regional Genetic Network (MSRGN) in order to establish regional networking, implement quality improvement projects and consumer input strategies, and support activities to improve access to genetic services within the region’s underserved communities. WY MCH’s Newborn Screening and Genetics Coordinator is currently serving a four-year term on the MSRGN Advisory Committee.
WY MCH continues to partner with Parents as Teachers National Center (PATNC), the MIECHV grantee in Wyoming, to build and support a network of home visiting organizations. In FFY19, WY MCH and PATNC met several times to discuss development of a Memorandum of Understanding (MOU) between organizations and coordination of the MIECHV and Title V NAs. Finalization of an MOU was delayed due to leadership changes and COVID-19 but is expected to be executed before fall 2020. To assure coordination of needs assessment activities, the MCH Unit Manager sits on the MIECHV NA Steering Committee and the Wyoming MIECHV Director sits on the Title V/MCH NA Steering Committee as well as relevant PATs. PATNC continues to offer key infrastructure support for the Wyoming Home Visiting Network, of which WY MCH is a member.
WY MCH continues to build workforce and systems capacity to address emerging needs through the offerings of the National MCH Workforce Development Center and the MCH Title V Internship Program. In summer 2019, the Child Health Program Manager applied for technical assistance to convene key statewide stakeholders within the Wyoming early childhood system to define the early childhood system, identify duplicate and complementary services, and identify gaps in available services. In summer 2020, WY MCH welcomed two graduate students as part of the MCH Workforce Development Center’s MCH Title V Summer Internship Program. The interns developed an MCH communications plan to assist in plans to better operationalize the unit’s core value of engagement.
Other Federal Investments
The Youth and Young Adult Health Program Manager partners with the Communicable Disease Unit to administer PREP.
WY MCH meets monthly with Wyoming Health Council (WHC), the Wyoming Title X grantee, to discuss current activities within both programs. Meeting topics have included a Reproductive Life Plan, Long Acting Reversible Contraceptives (LARC), and how the two programs can work together to improve family planning access throughout the state.
The CDC-assigned MCH Epidemiologist remains a member of the State’s Child Fatality Review and a member of its leadership council. WY CFR is currently led by the Wyoming Citizen Review Panel to review child maltreatment deaths and major injuries.
The Women and Infant Health Program Manager is the Office of Women’s Health representative and attends quarterly meetings that include state updates, resource sharing, and presentations responding to member inquiry and interest.
WY MCH benefits from an organizational structure that promotes collaboration with sister units of WIC, PHN, Immunizations, and Prevention and Health Promotion. Partnership with WIC includes promotion of statewide breastfeeding activities and development of improved lactation policies at WDH. WY MCH partners with PHN, WIC, and Immunizations to promote well visits through the Bright Futures Implementation Task Force.
Other HRSA Programs
Wyoming MCH continues to promote collaboration with the PHD Rural and Frontier Health Unit (RFH) through collaboration breakfasts, casual cross-unit meetings that offer staff an opportunity to learn about and partner with other HRSA-funded programs within RFH.
The Wyoming Primary Care Association (WYPCA) is another key partner of WY MCH and recipient of additional HRSA grants. WYPCA helped fill an important gap in statewide capacity to address oral health after the State-funded program was cut in 2016. WYPCA stepped in to lead the Wyoming Oral Health Coalition and recently joined a HRSA-funded oral health integration project (Rocky Mountain Network of Oral Health) focused on populations ages 0-40 months and pregnant women, with Denver Health serving as the lead agency. Additional HRSA grants administered or received by WYPCA include Primary Care Association grants and a new project with the Health Center Controlled Network with Community Healthcare Association of the Dakotas.
State and Local MCH Programs
WY MCH contracts with all 23 county PHN offices with combined funding of TANF and State General Funds provided for reimbursement of MCH services, such as home visitation and care coordination for CYSCHN. These funds fully or partially support an estimated 47 full-time employees across Wyoming in support of MCH services.
Tribes, Tribal Organizations, and Urban Indian Organizations
MCH tribal nurses serving both the Northern Arapaho and Eastern Shoshone tribes offer gap-filling financial assistance and care coordination services as part of CSH. CSH Benefits and Eligibility Specialists provide training and support to the nurses to improve and sustain programming.
The Wyoming PRAMS project continues to sample all births to Native American women. Wyoming PRAMS staff attend tribal health fairs and work with tribal health program leadership to provide data for review and use in tribal programs.
The Child Health Program Manager represents WY MCH on the Governor's Early Childhood State Advisory Council and the Wyoming Early Intervention Council. The MCH Unit Manager represents WY MCH on the Governor’s Developmental Disabilities Council.
III.C.2.c. Identifying Priority Needs and Linking to Performance Measures
The image below shows the process of selecting 2021-2025 priorities beginning with selecting NOMs (and additional emerging topics resulting from the SHA community meetings and MCH partner survey, if appropriate) and moving backward along a logic model continuum ending with finalized priorities and a State Action Plan, complete with selected/linked national or state performance measures and evidence-based strategy measures.

WY MCH focused its prioritization process on NOMs to assure alignment with the Title V performance measure framework and assure a limited number of resources were allocated to addressing priorities important both nationally and in Wyoming.
The figure below provides a high-level summary of the prioritization process.

{kind=link}
{kind=link}
{kind=link}
WY MCH cast a wide net to determine priorities to avoid biases in the selection process. Information on potential priorities was collected in three ways: SHA community meetings across the state, a survey of state partners, and a review of national and state health indicators of the MCH population.
As expected, WY MCH identified emerging issues for which MCH leadership role, capacity, feasibility, and/or political will was not sufficient enough for selection as a priority. Examples include mental health treatment for children, adequate insurance for children, and oral health. These topics will be further considered during the interim year needs assessments.
During this needs assessment process, three new emerging issues were identified and selected as new priorities - youth suicide, adolescent motor vehicle mortality, and maternal mortality - selected for their magnitude/burden in Wyoming when compared nationally (suicide and motor vehicle mortality) and for momentum due to new grants and capacity (maternal mortality).
To Top
Narrative Search